

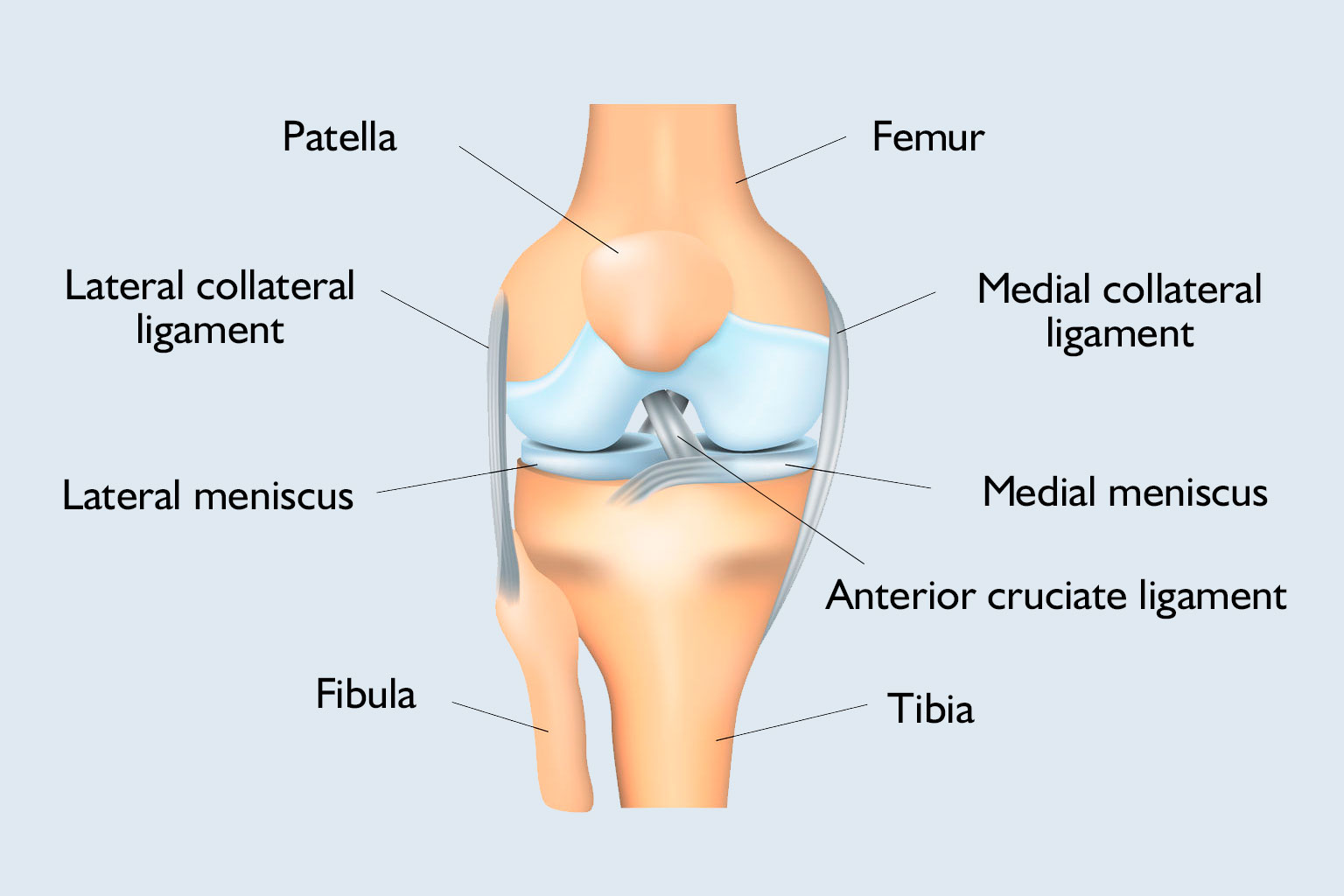
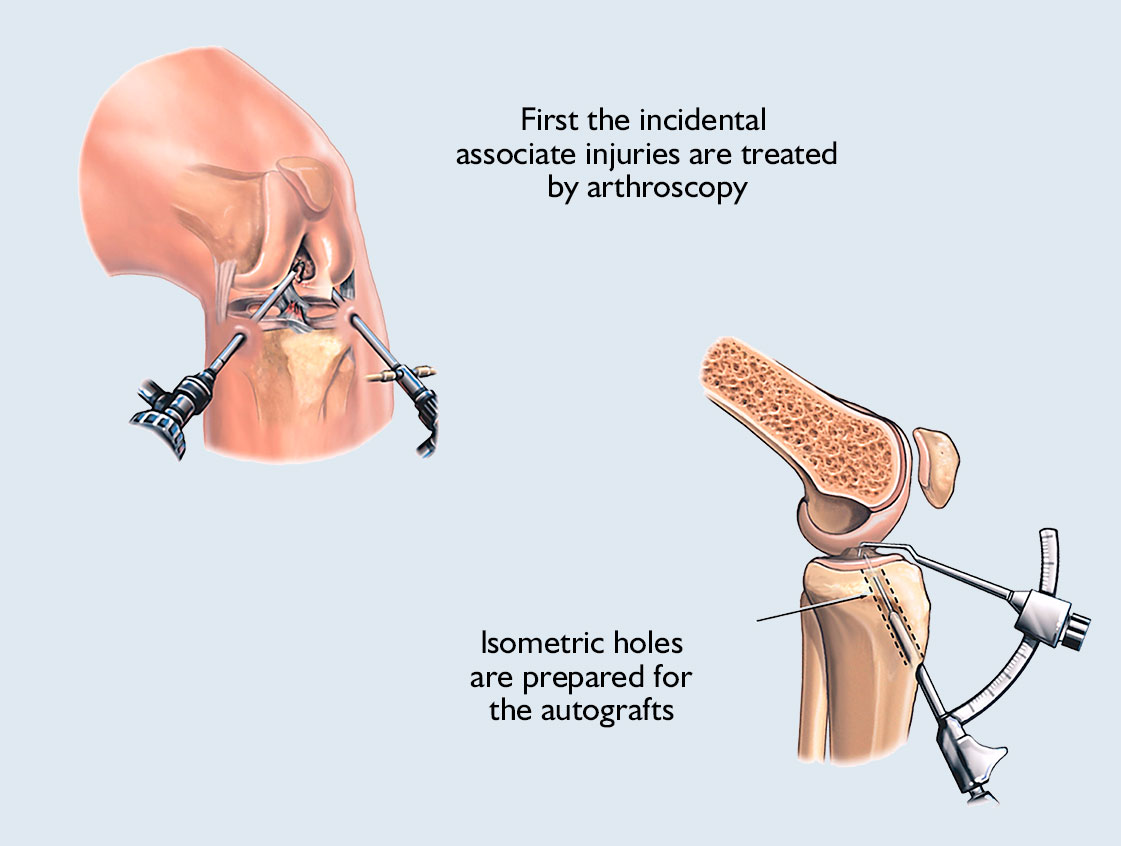
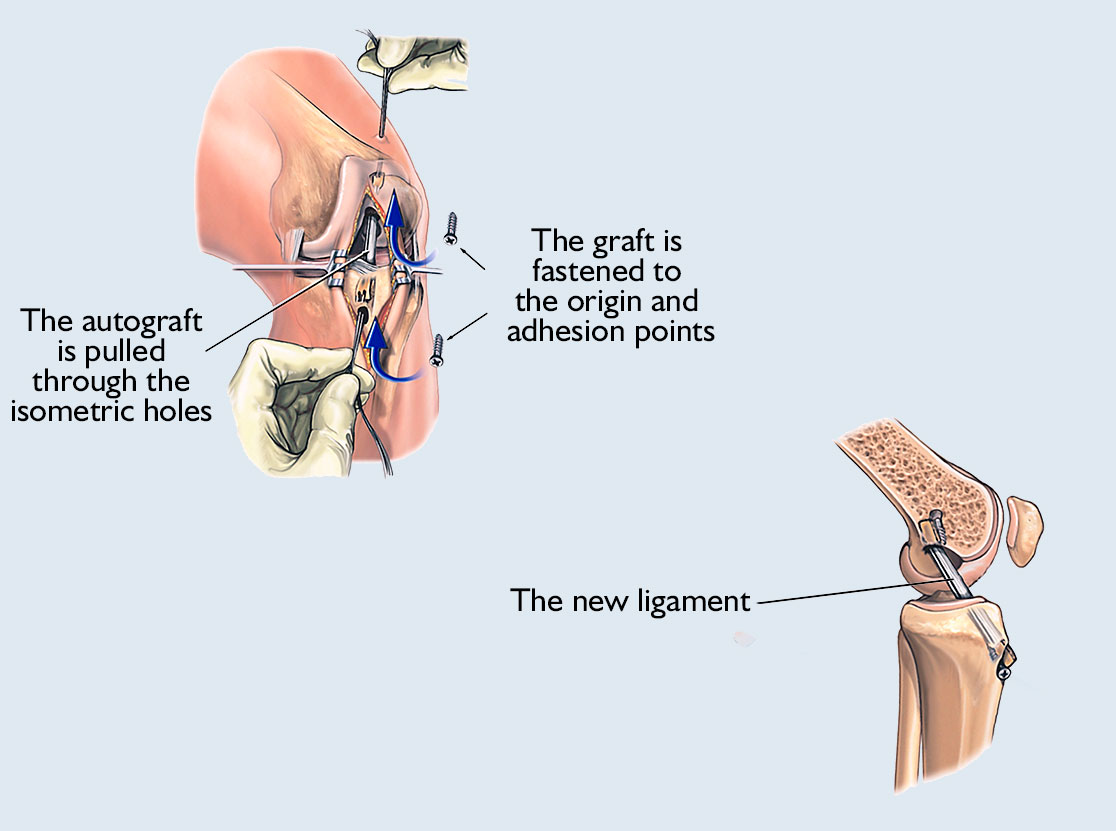
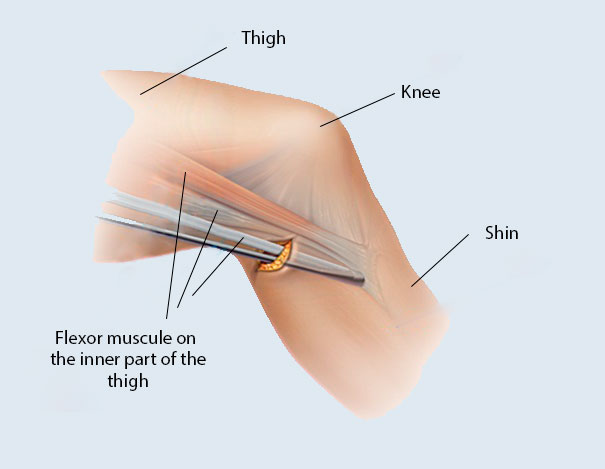
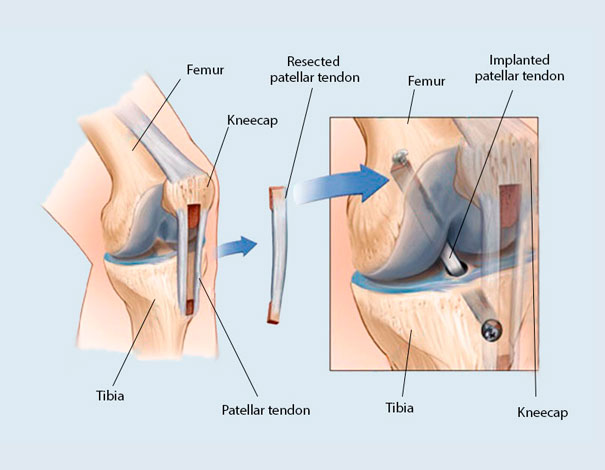
The injury of the anterior cruciate ligament is one of the most common knee injuries in sport. As the lesion of the ligament changes the kinematics of the knee joint, without treatment, it could cause degenerative defects too (meniscus injuries, wear of the joint surfaces). Anterior cruciate ligament surgery replaces the torn ligament with a tendon, usually from another part of the knee.
- Safety First COVID-19
-
Treatments
-
Orthopaedic Surgery
- Arthroscopic knee surgery
- Arthroscopic meniscectomy
- Anterior cruciate ligament (ACL) surgery
- Bunion surgery
- Carpal tunnel release
- Chondropathy surgery
- Cubital tunnel release
- Dupuytren’s contracture surgery
- Ganglion Removal
- Hammertoe surgery
- Hip replacement surgery
- Laser Disc Decompression (PLDD)
- Patellar dislocation
- Shoulder surgery
- Total knee replacement
- General Surgery
- Hand surgery
- Gynecological surgery
- ENT Surgery
- Ophthalmic Surgery
- Diagnostics
- Urological surgery
- Proctology
-
Orthopaedic Surgery
- Prices
- Our hospital
- Our Team
- Travel Guide
- Blog
- Contact
 info@mysurgeryabroad.com
info@mysurgeryabroad.com